
Signs You Might Have ARFID as an Adult (Not Just Picky Eating)

If you've been told your whole life that you're "just a picky eater" — but your eating patterns are affecting your health, relationships, or daily life — you might have something more than pickiness. You might have Avoidant/Restrictive Food Intake Disorder (ARFID).
ARFID is a recognized eating disorder where a person significantly limits the amount or types of food they eat — not because of concerns about body weight or appearance, but because of sensory sensitivities, lack of interest in food, or fear of negative consequences from eating. ARFID was officially recognized as a distinct eating disorder in the Diagnostic and Statistical Manual (DSM-5) in 2013, though it has been observed in individuals for much longer. ARFID is sometimes called selective eating disorder in older literature.
Between 1 and 5% of the population might have ARFID, affecting individuals of all genders and ages. Many adults with ARFID have never been ARFID diagnosed because the condition was only formally recognized in 2013. If you're reading this and thinking "this sounds like me," you're not alone — and help is available.
How Is ARFID Different From Just Being Picky?
The key difference comes down to impact. Everyone has food preferences. But ARFID becomes a clinical concern when your eating patterns lead to one or more of these consequences:
A clinical diagnosis of ARFID typically requires that food restriction leads to significant weight loss, severe nutritional deficiency, dependence on supplements or tube feeding, or marked interference with psychosocial functioning.
Here's what that looks like:
Normal picky eating: You don't like mushrooms, so you pick them off your pizza. You can still eat at restaurants, attend work events, and maintain a healthy weight.
ARFID: You can only eat 15-20 specific foods. You avoid dating because restaurants cause panic. You've been told you have iron deficiency anemia. You turn down job opportunities that involve client dinners.
The difference isn't about how many foods you eat — it's about whether your restricted food intake is creating real problems in your life.
How ARFID Is Different From Other Eating Disorders
Unlike anorexia nervosa or bulimia nervosa, ARFID is characterized by a limited eating pattern that can lead to significant medical and psychological consequences, and it is not motivated by a desire to lose weight or manipulate body shape. People with ARFID do not have negative body image or shape concerns driving their food restriction. If you have ARFID, your eating patterns are driven by the food itself — not by how you see your body.
In our work with adults who have ARFID, we've noticed that many people come in apologizing for "wasting our time" with their eating issues. They'll say "I know it's just being picky" or "I should be able to get over this." But ARFID isn't a willpower problem. When your eating patterns are causing weight loss, nutritional deficiencies, or preventing you from dating, attending work events, or maintaining relationships, that's a clinical issue that deserves professional support.
The Three Types of ARFID in Adults
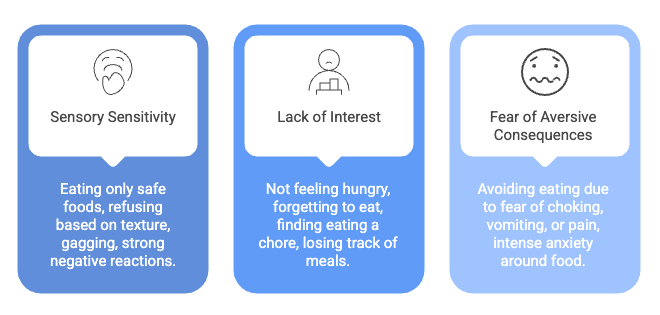
ARFID typically stems from three primary motivations: sensory sensitivity, fear of aversive consequences, and lack of interest. Many adults experience more than one type.
1. Sensory Sensitivity ("I Can't Stand Certain Textures, Smells, or Tastes")
This is the most common pattern. If you have sensory-based ARFID, you might:
Eat only 10-20 "safe" foods — the same items for years
Refuse foods based on texture, color, smell, temperature, or appearance
Be unable to tolerate certain foods touching each other on your plate
Gag or feel nauseated when trying unfamiliar foods
Have strong negative reactions or disgust to sensory characteristics of certain foods
Prefer bland, processed foods or very specific brands of accepted foods (if the brand changes, you can't eat it)
Have eaten this way for as long as you can remember
Research shows that food disgust plays a particularly important role in this pattern — the sensory qualities of certain foods trigger a strong aversion response that goes far beyond simple preference. Food disgust mediates the relationship between sensory sensitivity and picky eating, meaning that sensory sensitivity leads to disgust, which then drives the avoidant restrictive food intake.
2. Lack of Interest in Food/Low Appetite ("Eating Feels Like a Chore")
If you have this type of ARFID, you might:
Simply not feel hungry or forget to eat
Feel full very quickly after eating small amounts
Find eating to be a chore rather than a pleasure
Have to force yourself to eat
Lose track of meals throughout the day
Not understand why other people enjoy food or look forward to meals
Skip meals because eating food feels like too much effort
Miss hunger cues or not recognize when your body needs food
Recent brain imaging research has found that adults with this pattern show reduced activation in the hypothalamus (the brain's appetite center) when viewing food, suggesting a biological basis for the diminished drive to eat.
3. Fear of Aversive Consequences ("I'm Afraid Something Bad Will Happen If I Eat")
If you have fear-based ARFID, you might:
Avoid eating because you're afraid of choking, vomiting, having an allergic reaction, or experiencing pain
Have developed this extreme fear after a specific traumatic event (a choking episode, severe food poisoning, a medical procedure)
Feel intense anxiety before or during meals
Restrict your diet to foods you consider "safe" — often soft, bland, or familiar items
Avoid eating in public or social situations
Experience physical symptoms of anxiety (racing heart, sweating, nausea, upset stomach, or stomach cramps) around food
Research suggests that this pattern may have the best response to treatment, with studies showing that fear of aversive consequences is associated with higher likelihood of remission after two years compared to the other profiles.
We often see clients who have more than one ARFID profile at the same time. You might have sensory sensitivities to most foods AND a fear of choking from a past incident. Understanding which profile or combination drives your restriction helps us tailor treatment. Some people respond quickly to exposure-based work for fear, while sensory-based patterns often need slower, more gradual food introduction. There's no one-size-fits-all approach to ARFID treatment.
Warning Signs That Your Eating Might Have ARFID
Consider whether you recognize yourself in these patterns:
About Your Food Choices:
You eat fewer than 20 different foods eaten regularly
You've eaten essentially the same preferred foods for years or decades
The texture, smell, or appearance of most foods makes you feel disgusted or anxious
You can only eat specific brands of accepted foods (generic versions are intolerable)
You gag or feel nauseated when trying new foods
You categorize foods as "safe" and "unsafe" based on sensory qualities or fears
About Your Health:
You've experienced significant weight loss without trying, or you're underweight
You've been told you have nutritional deficiencies (low iron, low vitamin D, B vitamin deficiencies)
You rely on nutritional supplements like Ensure or protein shakes to meet basic needs
You experience fatigue, dizziness, hair loss, feeling cold all the time, or frequent illness
You have gastrointestinal symptoms or medical conditions that drive food avoidance
You're concerned you can't achieve expected weight gain even when trying
About Your Social and Professional Life:
You avoid social situations that involve food (dates, family gatherings, work events)
You've turned down job opportunities or promotions because they involve business meals
Dating feels impossible because of restaurant anxiety
Friends and family are frustrated by your eating habits or have stopped inviting you to meals
You feel isolated because food is central to most social activities
About Your Emotional Experience:
You feel anxious or distressed about eating food
You feel deeply embarrassed about your eating patterns
You've been told your whole life to "just try it" or "stop being so picky"
You feel shame that prevents you from seeking help
Eating causes physical anxiety symptoms (racing heart, sweating, panic)
How Common Is ARFID in Adults?
ARFID is more common than many people realize. Population-based screening studies suggest that approximately 1 in 4 adults screen positive for ARFID symptoms, though many of these cases may be milder. Clinical estimates suggest ARFID affects 1-5% of the general population at a level that causes significant impairment.
Approximately 9.2% of adults with eating disorders meet the criteria for ARFID, indicating its prevalence among adult populations. In adults, ARFID appears to be more common in women than men and more common in younger adults ages 18-39 than older adults 65+.
The average age of ARFID diagnosis is younger than for other eating disorders, with symptoms often beginning in early childhood. But many adults have lived with these eating patterns their entire lives without knowing there was a name for what they were experiencing.
What Causes ARFID? Risk Factors and Contributing Factors
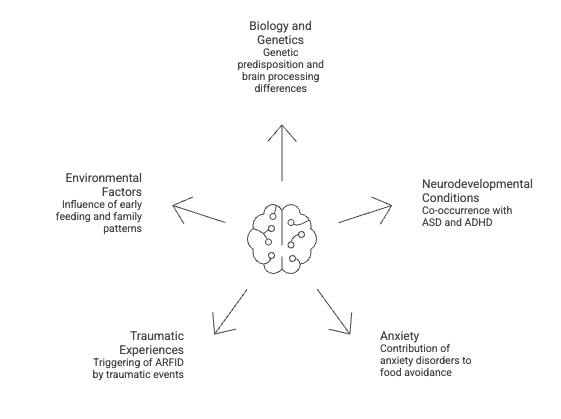
The exact causes of ARFID are not fully understood, but research points to several risk factors:
Biology and genetics. ARFID commonly runs in families, suggesting a genetic component. Brain imaging studies have identified differences in how the brains of people with ARFID process food-related information.
Neurodevelopmental conditions. ARFID frequently co-occurs with autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD). Sensory processing differences associated with these developmental disorders may contribute to food avoidance.
Anxiety. Anxiety disorders are among the most common mental health conditions that co-occur with ARFID. Generalized anxiety, social anxiety, and specific phobias can all contribute to and worsen food avoidance.
Traumatic experiences. A choking episode, severe vomiting, food poisoning, an allergic reaction, or a painful medical procedure can trigger ARFID, particularly the fear-of-aversive-consequences pattern, and trauma-focused cognitive behavioral therapy (CBT) can be part of addressing these experiences.
Environmental factors. Early feeding experiences, family eating patterns, and food availability during childhood can all play a role in the development of ARFID.
ARFID Often Comes With Other Mental Health Conditions
ARFID is highly comorbid with other mental health disorders, more so than anorexia nervosa or bulimia nervosa, often presenting with at least one additional mental health diagnosis. Individual therapy for depression and anxiety can be especially important, as common co-occurring mental health conditions with ARFID include autism spectrum disorder, ADHD, anxiety disorders, OCD, and depression, indicating a complex interplay of psychological factors.
Individuals with ARFID often experience heightened anxiety and sensory sensitivities, which can complicate their relationship with food and eating. In a large study of children with ARFID, researchers found that individuals had significantly elevated risk for 55 of 75 analyzed health conditions, with the highest risks for autism (10-fold higher), GERD, ADHD, anxiety, and mixed developmental disorders or other mental disorders.
Adults with ARFID also commonly have disorders of gut-brain interaction — ARFID-positive screens were significantly more common among adults with these conditions (34.6%) compared to those without (19.4%). Gastrointestinal symptoms and food avoidance can reinforce each other in a difficult cycle.
Why ARFID in Adults Often Goes Unrecognized
Many adults with ARFID have never been diagnosed for several reasons:
ARFID was only formally recognized in 2013. If you're over 30, you grew up when this diagnosis didn't exist. You were probably just labeled "picky" or "difficult."
Adults are expected to have outgrown pickiness. There's shame around still eating like a child, so many adults hide their eating patterns or avoid situations where their restrictions would be noticed.
ARFID doesn't look like typical eating disorders. Most people think eating disorders are about body image and weight loss. ARFID is different — it's not driven by concerns about body weight, shape, or appearance.
High-functioning adults can mask ARFID. If you're successful in your career, people assume you have your life together. You might meal prep your safe foods, avoid situations involving eating food, or use supplements to maintain functioning — but inside, you're struggling.
Healthcare providers may not screen for it. Even when you bring up eating difficulties, doctors may focus on weight or nutrition without recognizing the underlying feeding disturbance.
The most common thing we hear from newly diagnosed adults with ARFID is relief. After years of being told they're just difficult or stubborn about food, finding out there's a name for what they're experiencing — and that it's treatable — changes everything. Many of our Baltimore clients say they wish they'd known about ARFID sooner. The shame lifts when you understand this isn't a character flaw or something you chose.
The Health Consequences of Untreated ARFID
ARFID can have serious medical and psychological consequences for both physical and mental health.
Physical Health Impacts
Nutritional deficiencies are common with severely restricted diets. You may be lacking essential vitamins and minerals including:
Iron (leading to anemia and fatigue)
Vitamin D (affecting bone health)
B vitamins (affecting energy and nerve function)
Calcium (affecting bone density)
Zinc (affecting immune function and wound healing)
Protein (affecting muscle mass and overall health)
Weight loss or being underweight affects many adults with ARFID. In one study of adults hospitalized for ARFID, the average weight was only about 68% of ideal body weight — a level associated with serious medical complications. The most common laboratory abnormalities were low prealbumin and vitamin D, hypokalemia (low potassium), and leukopenia (low white blood cell count). Some adults maintain a normal weight by eating large quantities of a very limited range of foods — but they may still have severe nutritional deficiencies.
Medical complications of malnutrition can include low potassium (which can affect heart rhythm), low white blood cell count (increasing infection risk), low body temperature, slow heart rate (bradycardia), weakened bones (osteoporosis), muscle wasting, hormonal disruptions, and delayed puberty in younger adults.
Mental Health Impacts
Adults with ARFID have high rates of anxiety disorders and depression. These mental health conditions can both contribute to and result from restricted eating.
Social isolation is particularly difficult. Food is central to social life — meals with friends, family gatherings, work events, dating. When you can't eat what others eat, or when eating causes anxiety, you may withdraw from social situations. This isolation can worsen depression and anxiety.
Shame and embarrassment run deep. Many adults with ARFID feel deeply embarrassed about their eating patterns. They've been told their whole lives to "just try it" or "stop being so picky," leading to shame that prevents them from seeking help.
Research consistently shows that adults with ARFID symptoms have significantly lower mental and physical quality of life compared to those without ARFID.
When to Seek Help for ARFID
Consider talking to a healthcare provider or mental health professional if:
You eat fewer than 20 different foods regularly
You've lost weight without trying, or you're underweight and can't achieve expected weight gain
You rely on oral nutritional supplements (like Ensure or protein shakes) to meet your nutritional needs
You avoid social situations that involve food
You feel anxious or distressed about eating
You've been told you have a significant nutritional deficiency
Your restricted eating is affecting your relationships, work, or daily life
You experience physical signs that may be related to poor nutrition (fatigue, dizziness, hair loss, feeling cold all the time, frequent illness)
You have gastrointestinal symptoms that are driving food avoidance
You've had these eating patterns for years and they're not improving on their own
Getting an ARFID diagnosis can be the first step toward understanding and treating your eating patterns, and working with expert counseling in Baltimore can support you through that process.
How Is ARFID Diagnosed?
ARFID is diagnosed when a person has avoidant or restrictive eating behaviors that result in one or more of the following:
Significant weight loss (or persistent failure to achieve expected weight)
Significant nutritional deficiency
Dependence on nutritional supplements or tube feeding
Marked interference with psychosocial functioning (social life, relationships, work)
The diagnosis requires that the eating disturbance is not explained by:
Concerns about body weight or shape (which would suggest anorexia nervosa)
Lack of available food or food insecurity
Cultural practices (such as religious fasting)
A concurrent medical condition that fully accounts for the eating disturbance
Diagnosis typically involves a comprehensive evaluation including a detailed eating history, physical examination, laboratory tests like urine tests and blood work (to check for nutritional deficiencies), and psychological assessment.
Treatment for ARFID Works — Even for Adults
The good news: ARFID is treatable, and research shows that adults can make meaningful improvements.
Cognitive Behavioral Therapy is commonly used in ARFID treatment, focusing on changing negative thought patterns and behaviors related to food intake. In the largest study to date of 549 adults receiving CBT-AR (Cognitive-Behavioral Therapy for ARFID), ARFID patients demonstrated significant reductions in all three ARFID profiles, and those needing weight restoration gained an average of 0.34 pounds per week.
Treatment for ARFID often involves a multidisciplinary approach, including mental health professionals, dietitians, and therapists, to address the complex needs of individuals with the disorder. Successful recovery from ARFID typically involves a team of specialized professionals, including experienced therapists in Baltimore, dietitians, pediatricians or physicians, and occupational or speech therapists.
Recent research has demonstrated that CBT-AR can be effectively delivered through telehealth (video sessions), making ARFID treatment more accessible for adults who may not live near a specialized eating disorder program. Teletherapy with an online therapist has shown improvements comparable to in-person care across all ARFID symptom domains.
Key components of ARFID treatment include:
Establishing a regular eating schedule, typically three meals and two to three snacks daily
Creating low-pressure environments to reduce mealtime anxiety
Learning to manage anxiety around food and eating
Gradual exposure to new foods (for sensory-based ARFID)
Addressing fear through cognitive restructuring (for fear-based ARFID)
Building awareness of hunger cues and establishing healthy eating patterns (for lack-of-interest ARFID)
Early intervention is associated with improved outcomes. The sooner you seek help, the better your chances of recovery.
Finding ARFID Treatment in Baltimore
If you're an adult in Baltimore struggling with restricted eating patterns that are affecting your health or life, you don't have to keep living this way.
At the Baltimore Therapy Group, our therapists understand that ARFID is not about being difficult or picky — it's a real eating disorder with real consequences. We can help you understand your specific ARFID presentation, develop strategies to expand your food intake safely, manage anxiety around eating, address co-occurring mental health conditions, and work toward a more flexible relationship with food and healthy eating.
We serve clients throughout Baltimore, Towson, Roland Park, Canton, Fells Point, Mt. Washington, and surrounding areas, and can help you navigate in-person therapy options near you.
Schedule an appointment with the Baltimore Therapy Group today, or use our dedicated page to schedule therapy and counseling in Baltimore.
If you're experiencing a mental illness crisis or thoughts of self-harm: Call 988 (Suicide and Crisis Lifeline) for free, confidential support 24/7, or call the SAMHSA National Helpline at 1-800-662-4357.
Disclaimer: This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or qualified mental health provider with any questions you may have regarding a medical or mental health condition. If you are in crisis or experiencing thoughts of self-harm, please call 988 (Suicide and Crisis Lifeline) or go to your nearest emergency room.